Myofascial facial dysfunctions and their effect on aesthetic outcomes of botulinum therapy: a clinical and observational study
Authors
Yakovidi-Koneva Afina Stavrovna
Share
Annotation
The article summarizes information from open sources on the effects of facial myofascial dysfunctions, including myalgic and myofascial pain syndromes of the orofacial region, known as DC/TMD. These conditions can alter natural muscle patterns and, as a result, modify the response to neuromodulation. The article provides arguments in favor of the need for a preliminary assessment of the functional state of the musculoskeletal system and consideration of anatomical variability of facial muscles. Using the example of morphometric data of the frontal muscle, it is demonstrated how anatomical features can affect the results of neuromodulation. Documented cases of adverse events that may affect the visual effect and the subjective assessment of the result are also considered.
Keywords
Authors
Yakovidi-Koneva Afina Stavrovna
Share
Relevance of the study
The relevance of the study is explained by the fact that botulinum toxin injections are still one of the most sought-after and socially significant procedures in aesthetic medicine. According to professional statistical reports, botulinum therapy confidently occupies a leading position among non-invasive cosmetic procedures. Given the widespread use of the procedure, patients and practitioners strive for a predictable aesthetic result. However, in real clinical practice, variability in the effect is often observed, even when using similar protocols (doses, zones, and techniques), which makes it relevant to search for factors influencing the outcome.
Modern research shows that the result of botulinum therapy can be influenced by both the characteristics of injections (volume, dose, technique of administration and distribution of the drug) and the individual work of facial muscles. It is particularly interesting to consider the effect of facial myofascial dysfunctions on the outcome of the procedure. Changes in muscle tone, asymmetry of muscle contractions, the involvement of synergists and compensatory reactions can change the "map" of facial activity, which, in turn, affects the clinical response to neuromodulation. Indirectly, the importance of the functional-myofascial component is confirmed by the high incidence of myogenic disorders in the maxillofacial region, including painful forms of temporomandibular disorders, which makes them a likely cause of heterogeneity of aesthetic results.
Thus, the study of facial myofascial dysfunctions as a factor influencing the variability of aesthetic results of botulinum therapy is of great importance both from a scientific point of view (to understand the predictors of reaction and mechanisms of functional asymmetry) and from a practical point of view (to improve planning accuracy, reduce the number of repeated procedures and increase patient satisfaction, while maintaining natural facial expressions).
The purpose of the study
The purpose of this study is to understand how myofascial facial dysfunctions can affect the aesthetic outcome of botulinum therapy. We also want to identify elements of functional and anatomical assessment that can be included in clinical planning before the procedure in order to increase the predictability of the outcome.
Materials and research methods
The study used statistical data on the prevalence of aesthetic procedures, as well as documents regulating the use of BOTOX Cosmetic, including an analysis of adverse reactions identified in placebo-controlled trials. In addition, the consensus diagnostic criteria DC/TMD were applied, which describe myofascial and myalgic conditions in the orofacial region. Morphometric anatomical data on frontal muscle variability were also used.
The results of the study
Myofascial facial dysfunctions are disorders in the work of the musculoskeletal fascial complex of the maxillofacial region. These disorders cause changes in muscle tone and coordination, which leads to pain during exertion and palpation. In addition, areas of local muscle tension may form that maintain a stable "disadvantageous" motor stereotype. In the orofacial (maxillofacial) area, this approach is reflected in the diagnostic criteria of DC/TMD. According to these criteria, muscle pain conditions, including myalgia and myofascial pain with reflection, are described through the recurrence of pain characteristic of the patient during functional tests and standard palpation of the masticatory muscles and related structures [5].
In aesthetic medicine, it is important to understand that the facial and masticatory muscles are part of the multilayer structure of the soft tissues of the face. The superficial muscular-aponeurotic system (SMAS) is responsible for the mechanical connection between muscle contraction and the movement of skin and fat packets. Therefore, functional disorders in muscles and fascial ligaments can affect the formation of folds and asymmetry of facial expressions, as shown in Figure 1 [1].
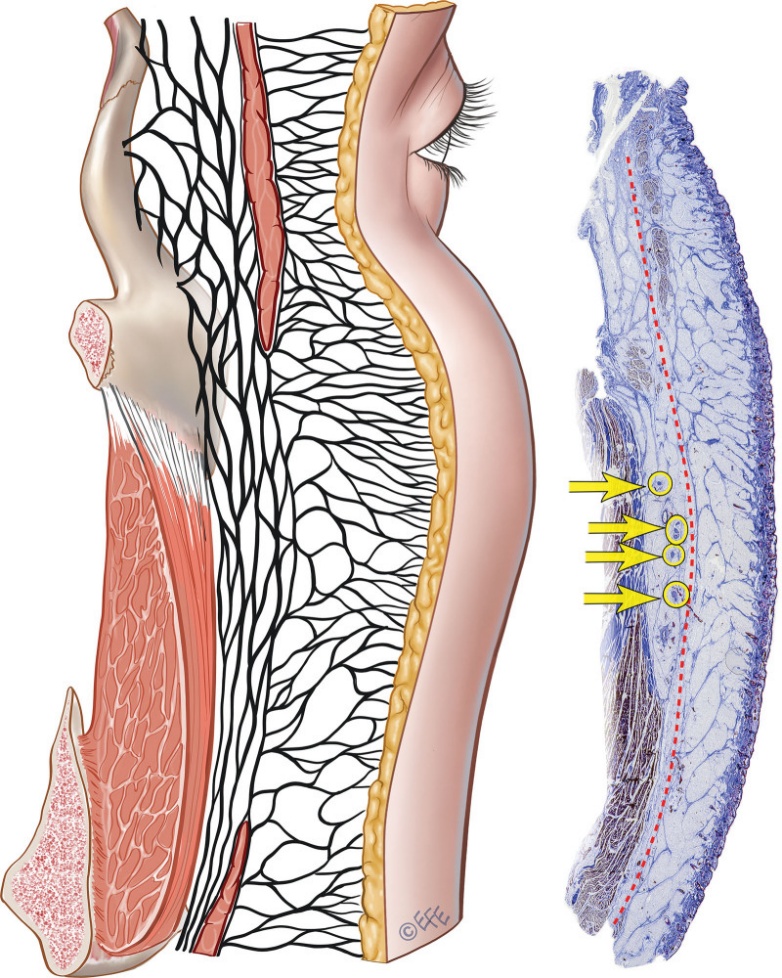
Fig. 1. Anatomical concept of SMAS and its relation to the soft tissues of the face [7]
Botulinum therapy is based on the action of botulinum toxin type A, which, entering the neuromuscular junction, blocks the release of acetylcholine. This, in turn, causes temporary "chemical denervation" and, as a result, a decrease in the activity of the target muscle.
Theoretically, the effect of facial myofascial dysfunctions on various aesthetic results of botulinum therapy can be explained by the fact that there is a discrepancy between the standard injection chart and the patient's actual functional chart. If the patient initially has an asymmetry of muscle tone, uneven load distribution on neighboring muscles, or stable patterns of hyperactivation or movement restriction, then even with the same dose and the same points of administration of botulinum toxin, there may be different visual results. In one case, botulinum therapy can lead to a harmonious decrease in hyperfunction, and in the other, to an increase in the relative dominance of unaffected muscles and noticeable asymmetry of facial expressions.
In addition, it is worth considering that open sources on the regulation of glabellar line treatment indicate different dosage regimens and efficacy indicators in key studies for different registered drugs. This indicates that the result is influenced by both the characteristics of the drug and the individual characteristics of the patient, among which myofascial status may be one of the key factors.
Clinical studies on aesthetic botulinum therapy usually emphasize the importance of standardized assessment of facial expressions and muscle movements prior to the procedure. The assessment includes examination of the face at rest and with different target expressions (for example, frowning, raising eyebrows, squinting), as well as photo and video recording under the same lighting conditions and head position. In addition, such studies usually demonstrate maps of facial muscles and typical areas of neurotoxin exposure. These maps can be useful to illustrate the differences between "anatomical landmarks" and "patients functional map" (see Figure 2).
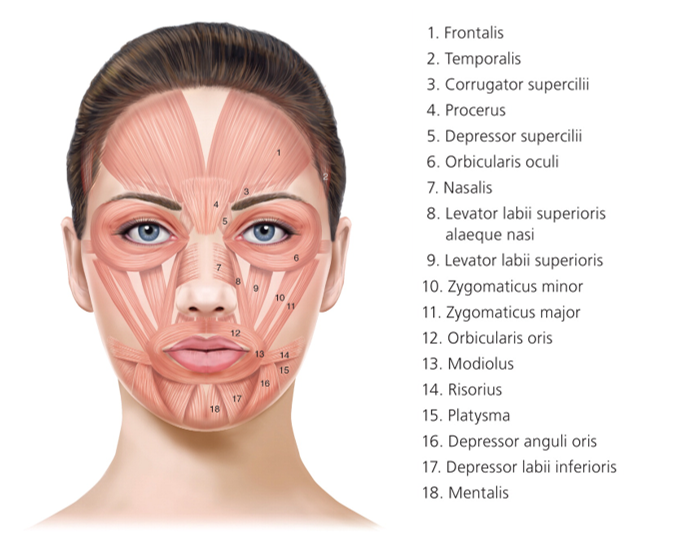
Fig. 2. Facial muscles [2]
If myofascial dysfunction affects the masticatory muscles and the temporomandibular region, then DC/TMD (Diagnostic Criteria for Temporomandibular Disorders) is recommended to describe a scientifically based diagnostic approach. This approach makes it possible to formalize muscle pain conditions based on a combination of medical history and clinical examination. It involves reproducing pain that is "familiar" to the patient with functional movements and palpation using standardized efforts (Table 1).
Table 1
Diagnostic accuracy of DC/TMD muscle pain diagnoses (sensitivity and specificity)
|
Diagnosis (DC/TMD, consortium publication) |
Sensitivity |
Specificity |
|
Myalgia (class of muscle pain) |
0.90 |
0.99 |
|
Myofascial pain with reflection (type of myalgia) |
0.86 |
0.98 |
A source: [4]
The safety and tolerability of botulinum therapy are also important aspects that need to be considered when discussing the variability of results. Patients as "poor aesthetic results" may perceive adverse events, even if the goal of reducing hyperfunction is achieved. The official instructions for BOTOX Cosmetic, a type A botulinum toxin preparation used to treat glabellar lines, contain a table of adverse reactions identified in double-blind, placebo-controlled trials. Facial pain (1%), facial muscle paresis (1%), upper eyelid ptosis (3%), and muscle weakness (1%) were noted among them. (Table 2).
Table 2
Adverse reactions in the treatment of glabellar lines: a comparison of BOTOX Cosmetic and placebo
|
Adverse reactions in the treatment of glabellar lines (BOTOX Cosmetic), more often than placebo |
BOTOX Cosmetic (N=405) |
Placebo (N=130) |
|
Pain in the face area |
6 (1%) |
0 (0%) |
|
Paresis of facial muscles |
5 (1%) |
0 (0%) |
|
Ptosis of the upper eyelid |
13 (3%) |
0 (0%) |
|
Muscle weakness |
6 (1%) |
0 (0%) |
A source: [8].
The issue of immunogenicity should be mentioned separately. Sometimes the decrease in the effectiveness of repeated procedures is explained by the "unpredictability" or "instability" of the result. The instructions for BOTOX Cosmetic indicate that the formation of antibodies is possible for protein preparations. In three studies on lateral canthal lines, binding antibodies were detected in 1.5% of the subjects, while no neutralizing antibodies were detected (0%). However, it is worth considering that comparing the frequency of antibodies between different studies and products is difficult due to limited analysis methods [8].
Aesthetic results of botulinum therapy can vary: from slight smoothing to complete symmetry of eyebrows and eyelids, as well as from complete immobility of facial expressions to its natural "liveliness". These differences largely depend on the initial condition of the facial and masticatory muscles, as well as the associated fascial structures. In clinical practice, this means that the same "morphological" request of the patient, for example, pronounced inter-brow or frontal dynamic wrinkles may have different musculofascial prerequisites. These prerequisites may include hypertonia of individual muscle bundles, asymmetry of muscle inclusion in facial expressions, the presence of trigger points and a pain component, as well as compensatory movement patterns. Myofascial pain syndrome and trigger points are a condition in which tense muscles form areas characterized by increased excitability. These areas can cause both local and reflected pain, as well as restrict motor functions.
This is especially true in the facial area, as the facial muscles are thin, attach close to the skin, and often work in concert. Masticatory muscles such as the masticatory and temporal muscles may be involved in myofascial disorders that may limit the functions of the temporomandibular joint. A study conducted on patients with dislocation of the TMJ disc (temporomandibular joint) showed that myofascial pain caused by trigger points in the masticatory muscles is associated with clinical symptoms and functional limitations [6].
To understand how botulinum therapy affects aesthetics, it is important to realize that its result is determined not only by the degree of relaxation of a particular muscle, but also by the overall balance of forces between antagonistic and synergistic muscles in this area. For example, if you focus only on the medial and central areas of the frontal muscle, without taking into account the lateral zones and the initial asymmetry, you may encounter an imbalance that will manifest itself as a rise in the lateral parts of the eyebrow with a relative weighting of the medial ones. Uneven relaxation of the frontal muscle can lead to deformation of the eyebrow line. In addition, it is important to take into account the myofascial characteristics of the patient: if a person initially has a different tone or degree of activity of the frontal and circular muscles of the eye, the compensations may be more pronounced, and even standard schemes of botulinum toxin administration may give results that are more diverse.
Table 3 shows real morphometric data reflecting the variability of the lateral extension of the frontal muscle and the distance from the so-called reference line (L2) to its lateral edge. These data were obtained as a result of a study of 49 hemilica.
Table 3
Morphometric parameters of the lateral extension of the frontal muscle and the distance to its lateral edge
|
Indicator (according to the research methodology) |
Result |
|
Lateral extension of the frontal muscle: presence of sections 2-5 in the range |
49 из 49 (100%) |
|
Lateral extension of the frontal muscle: presence of sections 2-6 in the range |
47 (95.9%) |
|
Lateral extension of the frontal muscle: presence of sections 2-7 in the range |
34 (69.4%) |
|
Lateral extension of the frontal muscle: presence of sections 2-8 in the range |
11 (22.4%) |
|
Lateral extension of the frontal muscle: presence of sections 2-9 in the range |
3 (6.1%) |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 1 |
5.6 ± 3.6 |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 2 |
3.7 ± 3.6 |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 3 |
3.9 ± 3.9 |
|
Average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 4 |
3.3 ± 3.7 |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 5 |
3.5 ± 4.0 |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 6 |
4.1 ± 5.8 |
|
The average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 7 |
4.3 ± 5.3 |
|
Average minimum distance from the L2 reference line to the lateral edge of the frontal muscle (mm), section 8 |
7.9 ± 4.0 |
A source: [3].
According to the conceptual model "myofascial dysfunction → outcome variability", anatomical features may enhance differences in the outcome of botulinum therapy. If the patient already has a functional asymmetry, for example, different involvement of the frontal and interbrow muscles, as well as compensatory hyperactivity of the circular eye muscle, soreness and trigger zones, then the final picture may be more pronounced against the background of anatomical variability of muscle boundaries.
In addition, patients with myofascial pain, for example, in the masticatory muscles, often experience changes in motor patterns, including protective ones. This can affect habitual facial expressions and tension in the periorbital area. As a result, the "expected" aesthetic effect at rest may not coincide with the effect of active facial expressions.
Conclusions
Thus, the variability of the aesthetic result of botulinum therapy depends on not only the injection parameters and characteristics of the drug, but also on the initial state of the patient's facial and masticatory muscles, which is determined by his myofascial status. The diagnosed myalgic and myofascial conditions of the orofacial region (in the context of DC/TMD) can maintain constant patterns of muscle tension and asymmetry, which can affect the visual response to neuromodulation and the subjective assessment of the result. Anatomical variability of the boundaries of facial muscles, as has been proven in studies of the frontal muscle, reduces the versatility of "protocol" methods and makes an individual approach more important. Even in official sources, undesirable phenomena are noted that directly affect appearance, for example, drooping of the eyelid after correction of glabellar lines during placebo-controlled studies. To increase the predictability of results, it is necessary to combine safety standards with a preliminary functional assessment of the musculoskeletal fascial complex and document outcomes.
References:
- Anatomy, Skin, Superficial Musculoaponeurotic System (SMAS) Fascia [Electronic resource]. – Access mode: https://www.ncbi.nlm.nih.gov/books/NBK519014.
- Botulinum Toxin Injection for Facial Wrinkles [Electronic resource]. – Access mode: https://www.aafp.org/pubs/afp/issues/2014/0801/p168.html.
- Characterizing the Lateral Border of the Frontalis for Safe and Effective Injection of Botulinum Toxin [Electronic resource]. – Access mode: https://pmc.ncbi.nlm.nih.gov/articles/PMC5127457/.
- Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group [Electronic resource]. – Access mode: https://pmc.ncbi.nlm.nih.gov/articles/PMC4478082/.
- Diagnostic criteria for temporomandibular disorders (DC/TMD): interexaminer reliability of the Finnish version of Axis I clinical diagnoses [Electronic resource]. – Access mode: https://pubmed.ncbi.nlm.nih.gov/28407454/.
- Do myofascial trigger points in masseter muscles affect the symptoms of disc displacement with reduction? A cross-sectional study [Electronic resource]. – Access mode: https://pmc.ncbi.nlm.nih.gov/articles/PMC10645171.
- The Superficial Musculoaponeurotic System: Does It Really Exist as an Anatomical Entity? [Electronic resource]. – Access mode: https://pmc.ncbi.nlm.nih.gov/articles/PMC11027987.
- This label may not be the latest approved by FDA [Electronic resource]. – Access mode: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/103000s5306lbl.pdf.
Other articles of the issue